

The last blogs dealt with the topic of lymphedema and its management. There is a similar but different condition known as lipedema-a disorder where the legs, and sometimes the arms will accumulate fatty tissue. It is often confused with obesity and many who have been diagnosed with obesity, may actually have lipedema.
Lipedema is an inherited disorder which unlike lymphedema occurs almost exclusively in women. The fatty tissue accumulates in the legs, but spares the ankle, and unlike fat cannot be lost by diet or exercise. It very often begins at puberty, but may also occur after pregnancy, in the perimenopausal period, following gynecological surgery, or even after any surgical procedure that requires general anesthesia.
Stress may also stimulate the development of lipedema, due to an increase in cortisol levels which cause inflammatory reactions, and trigger fat deposits.
There has been an estimate that up to 11% of post pubertal females have lipedema. Though the cause is unknown, there are genetically inherited risk factors at play, and the problem is more common in first and second degree relatives. There are also hormonal influences related to progesterone and estrogen imbalance.
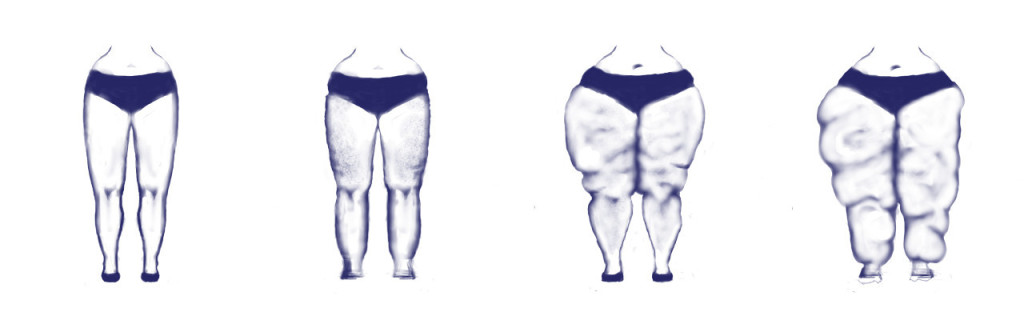
The symptoms of lipedema are disproportionately large legs, usually large to the level of the knees, as well as disproportionate hips, stomach, or buttocks. As the process progresses the patient becomes heavier in the lower body. The additional fat cells may interfere and compress the lymphatic channels causing lipo-lymphedema.
Unlike, those with lymphedema, these patients cannot tolerate the use of compression garments, because the lipedemic fat is very often painful, and as such these people may develop uncontrolled lymphedema, leading to fibrosis.
The treatment focuses, as with the treatment of lymphedema, in preventing progress of the process. These treatments include manual lymphatic drainage, best performed by certified therapist, as well as the use of compression hose where possible. These prevent recurrence of lymphedema, and in some patients reduce the pain related to lipidemic fat. Management includes reduction of sodium intake, frequent gentle exercises to increase the circulation of the legs. Many patients have succeeded in reversing the process through the use of elimination diets, low-impact exercises, and herbal protocols to prevent inflammatory reactions. Surgical management has been controversial, yet there has been some success with a procedure known as “water jet assisted” liposuction.
The best treatment is early diagnosis and management, as the process often begins in childhood.